







Patients often ask when they should have a hysterosalpingogram (HSG) to see if their fallopian tubes are open after tubal reversal surgery.
When to Have an HSG
Wait for at least 6 to 12 months after a tubal reversal procedure for this test of tubal patency. An HSG carries a risk of infection and often does not give conclusive results. It is best to give yourself a chance to become pregnant rather than rushing to have an HSG. Most patients conceive within this time frame and will avoid the need for an unnecessary and possibly misleading or harmful procedure.
Preparing for an HSG
To avoid unnecessary risks, an HSG should be performed only after menstruation is over and before ovulation occurs. Having an HSG after the time of ovulation may interfere with a pregnancy – before a pregnancy test can detect that conception has occurred. To minimize the risk of infection, use a betadine vaginal douche the evening before and the morning of the scheduled procedure and ask your doctor for a prophylactic antibiotic prescription. 600 mg of ibuprofen taken one hour before the HSG will minimize its discomfort.
What to Look For in an HSG
You can ask to watch the results on the fluoroscopy screen while the dye is being injected into the uterus.
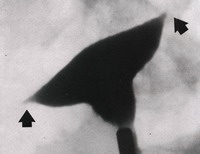 At first, the dye will fill the uterine cavity. It is essential that the dye actually enter the fallopian tubes up to the point where the anastomosis was performed. Often, this does not occur due to spasm of the sphincter between the uterus and tubes (shown by the arrows) or from mucus or calcium deposits in the proximal tubal segments.
At first, the dye will fill the uterine cavity. It is essential that the dye actually enter the fallopian tubes up to the point where the anastomosis was performed. Often, this does not occur due to spasm of the sphincter between the uterus and tubes (shown by the arrows) or from mucus or calcium deposits in the proximal tubal segments.
If the dye passes through the anastomosis sites, the fallopian tubes are open. Most radiologists do not consider the x-ray to show tubal patency (openness) unless dye spills into the abdominal cavity. When this happens, the diagnosis of tubal patency is conclusive.
We often see x-rays where dye has passed through the tubal anastomosis site, but has not yet spilled into the abdominal cavity. This is due to an insufficient amount of dye being injected into the tubes. The radiologist may mistakenly believe the tube is blocked when in reality it is open.
Send Your X-Rays To Me
In order to be certain about whether an HSG demonstrates tubal patency, tubal occlusion, or is inconclusive, please instruct the radiologist to send the x-ray films to me to interpret. Having documented the anatomy and measurements of the fallopian tube segments during tubal reversal surgery, I can compare the x-ray findings with each patient’s operative report. This allows me to give the most accurate interpretation of HSG results.
Dr. Monteith’s Comment
Hysterosalpingography is a widely available procedure to examine tubal anatomy. Unfortunately, it is often performed or interpreted inaccurately. An HSG also has risks as well as discomfort and cost. It is best to wait for at least 6-12 months after a tubal reversal procedure to have an HSG. Most patients will become pregnant after tubal reversal within a year and can avoid the problems associated with HSGs. Preparing properly for an HSG and sending the x-ray images to me will minimize the risks and errors associated with a hysterosalpingogram.

