







Optional Screening Laparoscopy Procedure
In our experience most tubal ligations can be reversed and provide women with a chance to become naturally pregnant. For patients who would like more reassurance about the chance of successfully repairing their fallopian tubes we offer an optional screening laparoscopy procedure.
What is a screening laparoscopy?
A screening laparoscopy is a surgical procedure which allows us to look directly at your fallopian tubes with a laparoscope (camera) inserted through a small incision. This procedure is performed under general anesthesia.
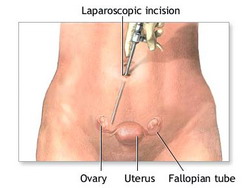 During a screening laparoscopy two small, 1/2 inch incisions are made on the abdomen: the first incision is made inside the umbilicus (belly button) and a second incision is made just above the pubic hair line. A camera is inserted through the first incision and a small grasper is inserted through the second incision.
During a screening laparoscopy two small, 1/2 inch incisions are made on the abdomen: the first incision is made inside the umbilicus (belly button) and a second incision is made just above the pubic hair line. A camera is inserted through the first incision and a small grasper is inserted through the second incision.
This allows a quick examination of the tubes to determine if they can be repaired before making a larger incision.
If the tubes can be repaired then a larger 3 to 4 inch tubal reversal incision is made above and parallel to the pubic hair line (mini-bikini incision) and the tubes are repaired.
If the tubes cannot be repaired then surgery is completed and band-aids are placed over the incisions.
Benefits of screening laparoscopy
A screening laparoscopy allows for a quicker evaluation of the fallopian tubes without making a larger incision. If the tubes cannot be repaired then the surgical time is shorter, there is less exposure to general anesthesia, a larger incision does not have to be made, and the surgical recovery is easier.
Since the surgical time is much shorter, patients who chose the laparoscopy will receive a significant refund of their surgical fee if their tubes cannot be repaired.
The fee for the optional screening laparoscopy is in addition to the tubal surgery fee.
Who should have a screening laparoscopy?
Laparoscopy not typically required when
One clip or ring has been placed each tube
Tubal ligation removed less than 3 cm of tube
Tubal coagulation performed with 2 to 3 burns close together
Uncomplicated Essure sterilization was performed
Laparoscopy should be considered when
Multiple clips or rings have been applied to each tube
Tubal ligation removed more than 3 cm of tube
Monopolar tubal coagulation was performed
Tubal coagulation involved more than 4 burns to each tube
No operative or pathology reports available for review
Multiple procedures performed on each tube
Fimbriectomy tubal ligation was performed
History of multiple (2 or more) c-sections or history of pelvic adhesions (scar tissue)
Essure with a history of previous multiple (2 or more) c-sections
Tubal ligations performed in the Caribbean or Latin America
C-sections and Scar Tissue: How can laparoscopy increase the chance of successful reversal?
C-sections can cause scar tissue in some patients. The more C-sections a patient has then the higher the chance of having scar tissue.
More information: Tubal Reversal and Scar Tissue: Should You Be Concerned?
 A screening laparoscopy can help increase the chance of a successful tubal reversal if severe scar tissue from C-sections is present.
A screening laparoscopy can help increase the chance of a successful tubal reversal if severe scar tissue from C-sections is present.
During a screening laparoscopy procedure, we can use an advanced Needle Localization technique to find the best area to make the abdominal incision, avoid severe scar tissue, and increase the chance of repairing both fallopian tubes.
Using this technique we can increase the chance of successful tubal repair when unexpected uterine scar tissue is present.
More information: Needle Localization and Screening Laparoscopy A Great Insurance Policy
Should you have a laparoscopy?
Screening laparoscopy can best be thought of as an insurance option. Any patient who would like a laparoscopy for more of a guarantee can have this procedure performed during their reversal surgery.
This information is intended as a general guide for our recommendations about when to consider a screening laparoscopy. We encourage you to send us copies of your operative and pathology records and our staff can help determine if a screening laparoscopy is appropriate. Always call us at (919) 977-5050 if you have questions.
Some patients will not be able to obtain copies of their tubal ligation records but many will come to our center and choose not to have laparoscopy with the reassurance we can repair most types of tubal ligations in the majority of our patients.
