Pelvic Endometriosis in Uncommon Locations
Diagnosed During Tubal Reversal Surgery
These are intra-operative photos I have collected during a 12-month interval of performing out-patient tubal ligation reversal surgery.
In all cases, no patient gave a history of endometriosis before tubal ligation and endometriosis was not diagnosed during the patient’s tubal ligation procedure. In all cases, the diagnosis of endometriosis was made by visual identification of typical endometriosis lesions and the visualized endometriosis was usually the site of tubal ligation. We do not routinely send tissue to pathology for confirmation because of cost concerns in a self-pay environment.
Deep nodular endometriosis after tubal coagulation
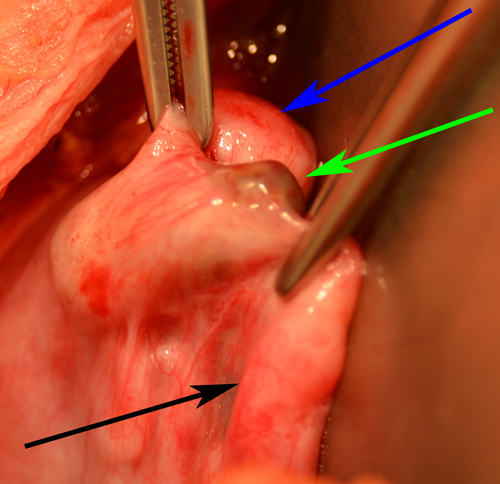
Deep nodular pigmented endometriosis, fibrosis, and adhesion formation
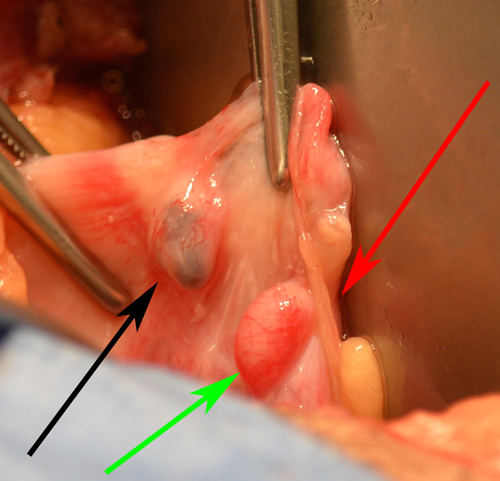
This patient had previously undergone tubal coagulation (tubal burning) as the method of tubal occlusion. Deep nodular, pigmented endometriosis was discovered underneath the proximal segment of fallopian tube. The white-ish appearance of the muscularis is suggestive of fibrosis and is commonly observed after tubal coagulation. The green arrow demonstrates a normal healthy appearing distal fallopian tube segment. The red arrow demonstrates an intestinal adhesive band to the mesosalpinx near the tubal ligation site.
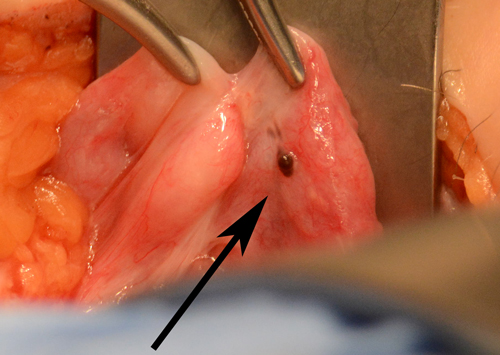
Superficial pigmented endometriosis of Broad ligament
Superficial pigmented endometriosis of Broad ligament
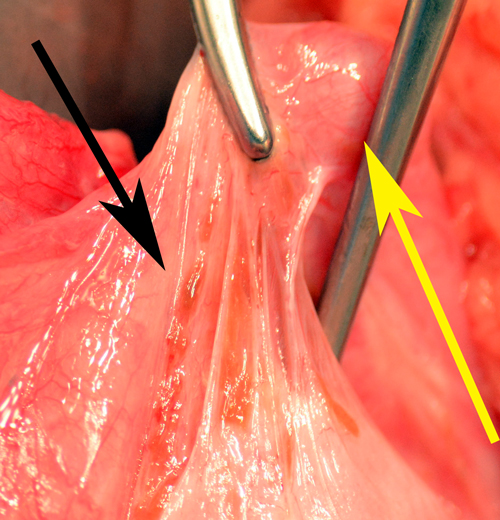
This patient had previously undergone a ligation and resection (cut and tie) method of tubal ligation.
During reversal surgery, we discovered superficial pigmented endometriosis on the serosal surface of the Broad ligament underneath the proximal tube.
The yellow arrow demonstrates the proximal tube and the black arrow demonstrates superficial endometriosis.
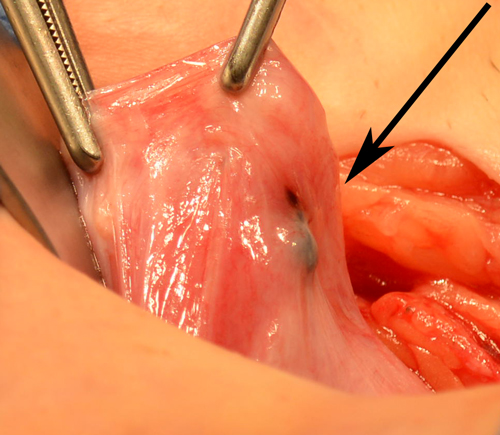
Both pigmented and non pigmented endometriosis of Broad ligament.
Superficial pigmented and non pigmented endometriosis
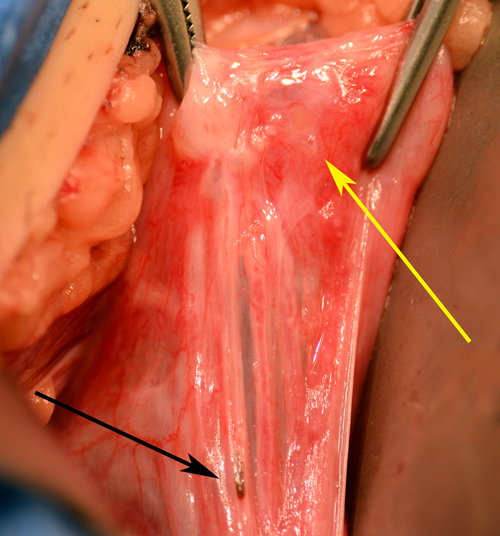
This patient had previously undergone a ligation and resection (cut and tie) type of tubal ligation. During reversal surgery, we discovered both superficial pigmented endometriosis and non-pigmented endometriosis on the serosal surface of the broad ligament underneath the distal segment of fallopian tube. The black arrow demonstrates superficial pigmented endometriosis. The yellow arrow demonstrates a superficial non-pigmented blister suggestive of non-pigmented endometriosis. This type of endometriosis can commonly be missed due to the lack of pigmentation, which assists in the visual identification of endometriosis.
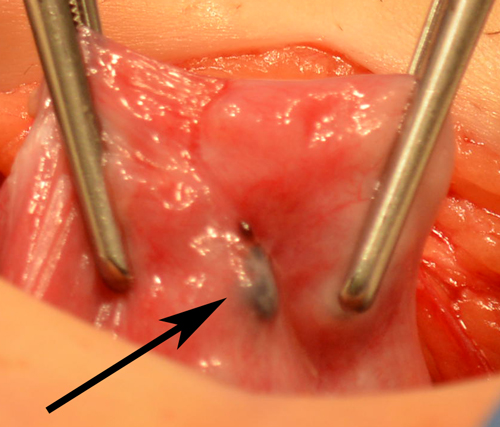
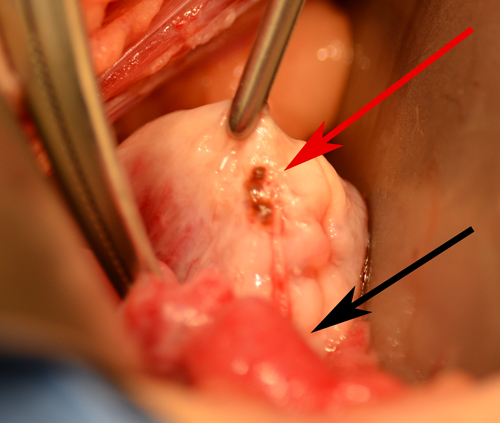
Deep pigmented endometriosis with surrounding fibrosis.
Deep nodular endometriosis and fibrosis
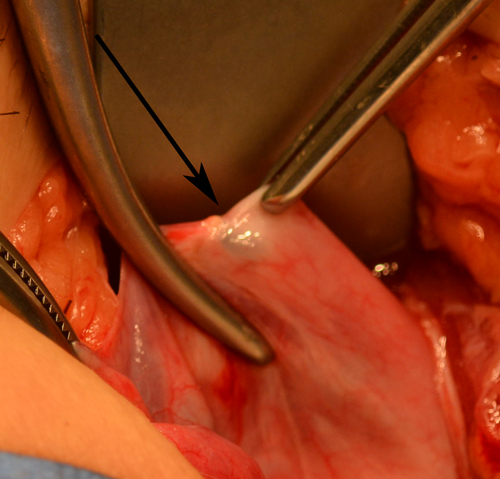
This photo demonstrates deep nodular, pigmented endometriosis involving the proximal segment of the fallopian tube. This endometriosis was deep and hard to visualize. The surrounding white fibrosis of the tubal muscularis is only visible when pressure is applied directly to the tubal segment. This causes a blanching effect presumptively due to compromised circulation as a result of the tubal ligation procedure.
This deep endometriosis and tubular fibrosis could easily be missed during a simple visual inspection.
Pigmented endometriosis with Filshie clip.
Pigmented endometriosis associated with tubal clip ligation
Although we commonly observe endometriosis with tubal coagulation and ligation and resection methods of tubal sterilization, we also have observed tubal endometriosis associated with tubal clips and tubal ring methods of tubal ligation.
This photo demonstrates a Filshie clip deeply embedded in the Broad ligament with surrounding fibrosis. The green arrow demonstrates the very end of the tubal clip with the dark pigment associated with endometriosis. Upon removal of the clip ‘dark chocolate fluid’ consistent with endometriosis was inside the tubal clip capsule.
The blue arrow demonstrates the proximal tube and the black arrow demonstrates the distal tubal segment.
 Isolated pigmented endometriosis and beginning of distal tubal segment
Isolated pigmented endometriosis and beginning of distal tubal segment
This photo demonstrates isolated pigmented endometriosis with healthy tubal segments and no visual evidence of fibrosis of the tubal muscularis.
The black arrow demonstrates endometriosis underneath the distal tubal segment.
 Deep nodular endometriosis inside Broad ligament
Deep nodular endometriosis inside Broad ligament
This patient underwent tubal coagulation (burning) type tubal occlusion.
The endometriosis was observed to be deep, nodular, and mostly inside the Broad ligament. The endometriosis is located underneath the mid-segment of the proximal fallopian tube as demonstrated by the black arrow.
 Pigmented nodular endometriosis
Pigmented nodular endometriosis
This patient underwent ligation and resection (tying and cutting) type tubal occlusion.
Nodular, pigmented, deep infiltrative endometriosis was observed underneath the distal tubal segment. This is often removed during the tubal repair and during removal ‘chocolate type fluid’ associated with endometriosis is often discovered.
 Ovarian endometriosis observed during tubal reversal surgery
Ovarian endometriosis observed during tubal reversal surgery
Pigmented superficial endometriosis was observed on the ovarian capsule during tubal reversal surgery. This patient had previously undergone a ligation and resection type of tubal ligation.
The red arrow demonstrates the isolated endometriosis on the ovarian capsule. The black arrow demonstrates the distal fallopian tube.
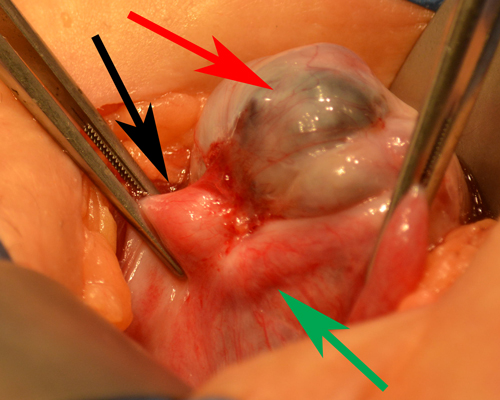
Ovarian endometrioma adherent to the site of tubal ligation.
Ovarian endometrioma adherent to tubal ligation site
This patient had undergone ligation and resection (tying and cutting) type of tubal ligation. She was observed to have normal pelvic anatomy at the time of tubal ligation and she did not have a history of endometriosis before her tubal ligation.
At the time of tubal reversal she was discovered to have an ovarian cyst containing endometriosis (endometrioma).
The red arrow demonstrates the endometriomal cyst wall. This endometrioma was estimated to be 3cm in diameter. The red arrow and green arrow demonstrate the proximal and distal tubes. The ovary is adherent to the tubal ligation site and there is extensive thickening of the tubal muscularis with reactive fibrosis.
During surgery, the ovary was removed from its attachment to the tubal segments. The endometrioma cyst wall was removed, the fibrotic tubal ends resected, and tubal anastomosis was subsequently accomplished without difficulty.
