







Tubal Reversal Procedures
There are 3 types of tubal reversal procedures:
- anastomosis
- implantation
- salpingostomy – (this topic)
Salpingostomy Definitions
Salpingostomy is creating an opening in the fallopian tube. It is also called neosalpingostomy, which more clearly indicates the creation of a new opening in the tube. Salpingostomy is the appropriate tubal reversal procedure when the end closest to the ovary is closed and the fallopian tube has not been divided into separate segments. This is what results from a fimbriectomy tubal ligation. It can be seen also when a fallopian tube has become closed as a result of infection (salpingitis).
How I Perform Ampullary Salpingostomy
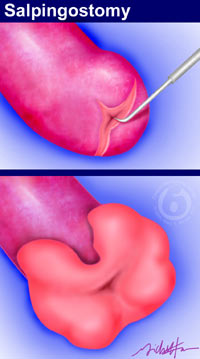 Salpingostomy involves creating an opening in the end of the fallopian tube with a microsurgical needle electrode. The opening is enlarged and gently folded back so that the internal lining extends over the opened end of the tube. The internal lining is covered with cilia, the hairline projections that beat in coordinated waves. They help capture an egg as it is released from the ovary just as the fimbrial end of the tube does normally. Sutures are placed around the end of the tube that has been folded back. The sutures are hidden underneath the folded-back tubal end. When ampullary salpingostomy is completed, the tubal end looks similar to a normal fallopian tube, provided there is a sufficient ampullary length of tube remaining to fold back.
Salpingostomy involves creating an opening in the end of the fallopian tube with a microsurgical needle electrode. The opening is enlarged and gently folded back so that the internal lining extends over the opened end of the tube. The internal lining is covered with cilia, the hairline projections that beat in coordinated waves. They help capture an egg as it is released from the ovary just as the fimbrial end of the tube does normally. Sutures are placed around the end of the tube that has been folded back. The sutures are hidden underneath the folded-back tubal end. When ampullary salpingostomy is completed, the tubal end looks similar to a normal fallopian tube, provided there is a sufficient ampullary length of tube remaining to fold back.
Types of Salpingostomy
The type of salpingostomy is specified according to the tubal segment that has been opened. This will depend on how much of the fallopian tube was removed during a fimbriectomy. The illustration above shows an ampullary salpingostomy. Salpingostomy at the ampullary, infudibular, or fimbrial tubal segments can result in good success rates. If a large amount of tube has been removed and only the isthmic segment remains, salpingostomy is unlikely to result in pregnancy.
Comment About Salpingostomy
The success of salpingostomy for fimbriectomy tubal reversal depends upon having an adequate length of ampullary segment of the fallopian tube. The length of the remaining ampullary tubal segment can be determined from a hysterosalpingogram (HSG) or from diagnostic laparoscopy. I recommend having an HSG or choosing the screening laparoscopy option when tubal ligation has been performed by fimbriectomy. An HSG can be ordered by the patient’s local doctor and the x-ray films sent to me for examination prior to scheduling tubal reversal surgery. Alternatively, patients can omit having an HSG and schedule their reversal surgery to start with screening laparoscopy. This will show if ampullary salpingostomy will be effective. If so, the tubal reversal procedure will be performed at the same time while the patient is under anesthesia.

