







Contrary to what most health care providers believe…you can reverse Essure. You can become naturally pregnant after Essure reversal.
We specialize in Essure reversal and Essure removal. We have extensive experience with removing Essure and tubal ligation reversal.
 We were the first doctors to remove Essure devices and publish our results in the medical literature.
We were the first doctors to remove Essure devices and publish our results in the medical literature.
In 2008, we started helping women who were having problems with the Essure device. These devices were new and most doctors did not know how to deal with Essure complications. These women would contact our office because most other doctors were not willing to admit the Essure devices were causing problems.
Patients traveled to us from across the United States for Essure reversal (to get pregnant) and removal surgery (to treat symptoms). Some of these women had problems from the devices. Many others regretted their decision and wanted to have more children.
Many of our patients will take 1 to 2 years to make the decision to have surgery. They often spend this time researching who is the best doctor, where is the best place for surgery, and what are the chances of pregnancy after Essure reversal.
A common question we are asked is, “Do you need a c-section after Essure reversal surgery?”
If you ask us do you need a c-section after Essure reversal our response will be…you only need to do two things in life: die and pay taxes! Having a c-section is not on the list of mandatory life events.
We recommend our patients have a planned c-section for any future pregnancy after Essure reversal surgery.
Some doctors tell patients they can have a vaginal birth after reversal without any concerns. We believe it is safer for moms who become pregnant after Essure reversal to have a planned c-section before going into labor.
With reversal of most tubal ligations the incisions are made on the fallopian tube… these patients do not need a c-section. Essure reversal and removal require that an incision be made into the uterine muscle.
We will share our considerable experience and advice about the safest way to deliver a baby after having Essure reversal surgery.
Who needs a c-section?
Deciding who needs a c-section is not straightforward. There are many reasons why you may need a c-section.
In the United States, the three most common reasons for needing a c-section are:
- Fetal distress in labor
- Cervix not dilating
- History of a previous c-section
If you would like to see a more comprehensive list of reasons for needing a c-section then you should visit the Mayo Clinic’s website which gives a nice review of the reasons for needing a c-section: C-section: Why it is done?
The last reason on the Mayo Clinic’s list for having a c-section is relevant to this conversation about c-sections after Essure reversal:
You’ve had a previous C-section or other surgery on the uterus. Although it’s often possible to have a vaginal birth after a C-section, a health care provider might recommend a repeat C-section.
Why is this relevant to pregnancy after Essure reversal?
Incisions made into the uterus weaken the uterus
Any previous surgery on the muscle of the uterus can weaken the uterus and make it more prone to tearing or rupturing in a future pregnancy. The uterus is a muscle. Muscle tissue does not heal as well as skin, bones, or even tendons. Muscle tissue will always be weaker after making an incision in the uterine muscle and after the tissue heals back together.
Any person who has torn their bicep muscle, hamstrings, or even Achilles tendon knows it is hard…if not impossible…to heal 100% after such an injury. These injuries are often career ending for many professional athletes. The same is true of the uterus after an incision has been made in the uterine muscle.
The uterus will always be weaker after an incision is made into the uterine muscle.
C-section and vaginal birth after c-section: What’s the concern?
The concern with having a vaginal birth after c-section is you could have a uterine rupture. To put it bluntly, it is possible your uterus could rip open while you are in labor. If this happened it would be in the same area where the incision was made on your uterus.
Remember, the uterus is a muscle. Once muscle tissue has been cut it never heals as strong as it was before the cut was made.
 Just like a balloon popping, most ruptures of the uterus happen when the uterus is under maximal stress. This most commonly happens while you are in labor or within the last several weeks of pregnancy when the uterus is distended in the third trimester.
Just like a balloon popping, most ruptures of the uterus happen when the uterus is under maximal stress. This most commonly happens while you are in labor or within the last several weeks of pregnancy when the uterus is distended in the third trimester.
The uterus is a dynamic organ. When you are not pregnant the uterus is the size of a human fist. When you are pregnant in the last trimester your uterus would have grown to the size of a small watermelon.
This change, growth, and stretching of the uterus puts stress on the incision and could cause the incision to tear open at anytime during the pregnancy. This most commonly occurs in the least several weeks of pregnancy…or while the uterus is forcefully contracting when you are in labor.
So the concern with a future pregnancy after you have had an incision on your uterus is that your uterus could rip open. If this happens it can be anytime during a pregnancy. It happens most often when you are in labor but it can also happen during the third trimester.
What happens if you have a uterine rupture?
A rupture of the uterus is a major complication of pregnancy. If rupture is diagnosed in time then you may not have any problems. If uterine rupture is not diagnosed in time the results but can be devastating.
These are the risks of having a rupture of the uterus:
- You may need an emergency C-section
- You may need a blood transfusion
- You may need a hysterectomy at the time of your C-section
- The umbilical cord or placenta could be compromised and the baby not get enough blood flow or oxygen
- The baby could be born with brain damage
- You or the baby could die in labor
In the United States it is very rare for a mother to die from uterine rupture. Fetal death or birth injury are more common.
Uterine ruptures can be sudden and catastrophic. Your doctor may not be able to perform an emergency C-section in enough time to save you or the baby from having a problem.
What is the chance of uterine rupture?
Most of our information about uterine rupture comes from c-section data. There have been hundred of thousands of c-sections performed over the last 50 years. In comparison, there have been just a few hundred Essure reversal surgeries.

Low transverse uterine incision: Lower part of uterus
The chance of uterine rupture depends on where the incision was made on the uterus during the c-section: the lower uterine segment or the upper uterine segment.
Please keep in mind…when we are talking about incisions made on the uterus.
We are not talking about how the incision was made on your abdomen. We are talking about the type of incision made on the uterus only.
Side-to-side uterine incisions
The safest place to make a C-section incision is the lower uterine segment because the area above the cervix is less muscular and less prone to rupture.
Usually this is a ‘side-to-side’ incision that goes from one side of the uterus to the other. This incision is in the part of the uterus that stretches open with the cervix but is not as muscular. The chance of uterine rupture is less in this area.
A low ‘side-to-side’ incision on the uterus is often called a low transverse uterine incision.
If you put your uterus through the maximal stress test…that is trying to have a vaginal birth after a previous low ‘side-to-side’ c-sections then your risk of uterine rupture is less than 2%.
For more information: Risk of uterine rupture during labor among women with a prior Cesarean delivery
‘Up and down’ or vertical uterine incision
The worst place to make an incision is in the upper part of the uterus. This is the thickest part of the muscle.
Vertical uterine incision: Upper and lower part of uterus
This area does not always heal back to full strength. These incisions cause more weakness in the muscular wall of the uterus. Usually these are ‘up-and-down’ incisions. They are commonly called Classical or vertical uterine incisions.
The incision that are made in the thickest part of the uterine muscle often occurs during a Classical c-section for a preterm infant.
The term classical is because in the very early days of c-sections…all uterine c-section incisions were classically made up and down. It was considered the standard way to perform a c-section until doctors realized these incisions caused more complications in future pregnancies.
If you have a previous ‘up-and-down’ incision on your uterus and you put your uterus through the maximal stress test…that is trying to have a vaginal birth after a previous Classical or vertical incision c-section, then the risk of rupture of the uterus can be as high as 12%…or 1 out of 10 pregnancies.
For more information: Uterine Rupture Risk After Periviable Cesarean Delivery
Most doctors today do not make vertical uterine incisions during c-sections unless the baby is preterm.
Again…the discussion about type of incisions are about how the incision was made on the uterine muscle and not the visible skin incision made on your abdomen.
What does this have to do with Essure Reversal?
To some extent the above information has NOTHING to do with Essure reversal but the concerns of uterine rupture have EVERYTHING to do with pregnancy after Essure reversal.
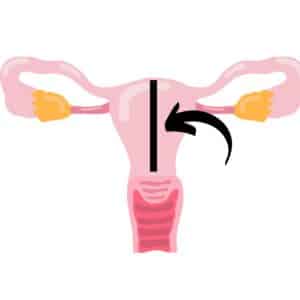
The Essure devices are inserted into the very opening of the fallopian tubes as these tubes travel through the thickest part of the uterine muscle…in the upper part of the uterus.

Essure reversal incisions: Upper part of uterus
The only way to remove and reverse Essure is to make incisions on each side in upper part of the uterine muscle which is the thickest part of the uterine muscle.
Small incisions are made into the thickest part of the muscle, the devices are removed, and the tubes are reinserted back into the uterine muscle.
There really is no other way to do it….you dont have to be a doctor to understand this.
The concern is Essure reversal requires incisions in the part of the uterus known to not heal as well as other parts of the uterus.
Incisions in these areas generally have a higher chance of uterine rupture in a future pregnancy.
What is the chance of uterine rupture after Essure reversal?
There are no good medical studies describing chance of uterine rupture after Essure reversal. Why?
Essure reversal is not common. There are not enough Essure reversals done in the entire United States to give us enough information on what the chance of uterine rupture is after reversal of Essure.
The few doctors who offer Essure reversal do not keep comprehensive statistics or have good enough follow-up with their patients to determine the actual risk of uterine rupture. If they do have good follow-up they have not published their results.
First to publish results of reversing Essure
We were the first to publish peer reviewed research papers on the possibility of pregnancy after Essure reversal.
- Normal pregnancy after outpatient tubouterine implantation in patient with Adiana sterilization
Monteith, Charles W. MD; Berger, Gary S. MD, MPH, Fertil Steril: July 2011 – Volume 98 – Issue Part 1 – pages e45-e46 - Successful Pregnancies After Removal of Intratubal Microinserts
Monteith, Charles W. MD; Berger, Gary S. MD, MPH, Obstetrics & Gynecology: February 2012 – Volume 119 – Issue Part 2 – p 470–472 - Pregnancy Success After Hysteroscopic Sterilization Reversal
Monteith, Charles W. MD; Berger, Gary S. MD; Zerden, Matthew L. MD, MPH, Obstetrics & Gynecology: December 2014 – Volume 124 – Issue 6 – p 1183–1189
The point we are trying to make is we took the time to document our procedure and track our success and failures.
We maintained follow up with our patients to be aware of what was happening. We also took the time to write and publish research papers.
This requires a great deal of effort but we felt it was important to let doctors know that Essure reversal and pregnancy were possible.
Essure reversal: Pregnancy outcome and chance of uterine rupture
 We were very concerned about the risk of uterine rupture in our Essure reversal patients.
We were very concerned about the risk of uterine rupture in our Essure reversal patients.
So we thought it was best and safest to recommend all our patients have a c-section. Essentially, we thought it best “to be safe rather than sorry.”
Between January 2009 and January 2017, we performed 253 bilateral tubouterine implantation procedures (Essure reversal surgeries).
Essure reversal results: Of these 253 patients, 100 patients self-reported pregnancy by natural conception. These 100 patients reported 131 pregnancies; 95 live births, 23 miscarriages, and 4 ectopic pregnancies. The outcomes for 9 pregnancies were unknown.
Risk of uterine rupture. Of the 95 pregnancies reported above, four (4) patients reported uterine rupture after surgical reversal of Essure sterilization. So the risk of uterine rupture was about 4%.
Cases of uterine rupture after Essure reversal
Patient #1. Her first pregnancy after Essure reversal was delivered by scheduled cesarean delivery at 39 weeks without complication. During her second pregnancy, she experienced a uterine rupture at 37 weeks gestation, underwent an emergent cesarean delivery, and required a blood transfusion. Her baby was admitted to the NICU, diagnosed with Hypoxic-Ischemic Encephalopathy, and underwent neonatal cooling therapy. The baby remained in intensive care for 3 weeks.
Patient #2. After 12 hours of painful contractions, she experienced gradually increasing abdominal pain at 36 weeks gestation. She underwent cesarean delivery and was diagnosed with a uterine rupture. The patient required blood transfusion; however, neither mom nor baby experienced a significant complication. This patient had a second pregnancy and had cesarean delivery without complication.
Patient #3. After reporting abdominal pain, she underwent emergency cesarean delivery and was diagnosed with uterine rupture at 36 weeks. Neither mom nor baby experienced a significant complication.
Patient #4. This patient was diagnosed with an asymptomatic uterine rupture during a scheduled cesarean delivery at 36 weeks. During the cesarean, her doctor discovered a 2 cm asymptomatic uterine window near one of the tubal implantation sites. Neither mom nor baby experienced a significant complication.
If you would like to see our advice regarding the risk of Essure reversal then visit: Pregnancy risks of reversing Essure sterilization
Chance of uterine rupture in our patients
The risk of uterine rupture was about four (4) women out of every 95 live births…or about 4%.
Please keep in mind…these were patients who we communicated to both patients and their doctors to plan a c-section before going into labor. Most of the other patients who did not have uterine rupture had planned c-sections between 35 to 39 weeks.
The point we are trying to make is if we told all patients they could have a vaginal birth the risk of rupture could have been much higher. These women would have tried to extend their pregnancies several weeks and also tried to labor. The uterine rupture risks could have increased during this time and been higher than 4%.
This is one reason we elected to be cautious in our recommendations to our patients.
What we are trying to caution readers is this: Our risk of uterine rupture was about 4% which is low but not insignificant.
If we have told all our patients it was okay to have a vaginal birth and they stressed their uterus out by going into labor then the uterine rupture number could have been much higher.
It could have been as high as 10% to 15%, which is a significant percentage when you are talking about something as serious as a rupture of the uterus.
Do you need a c-section when reversing Essure? Playing the math game
We have a lot of experience with Essure reversal and because of these we generally know what we are talking about. Let’s play a math game.
 We have observed the chance of pregnancy is about 40% after Essure reversal. Lets assume the risk of uterine rupture is 5 %.
We have observed the chance of pregnancy is about 40% after Essure reversal. Lets assume the risk of uterine rupture is 5 %.
This means for every 100 Essure reversal surgeries you do about 40 patients will become pregnant. Some will miscarry…so lets say you need to do 120 Essure reversal surgeries have 40 patients get pregnant, not miscarry, and carry to term.
- This means a doctor would have to do about 300 Essure reversal surgeries to have 120 pregnancies.
- Of the 120 pregnancies, some of these pregnancies will miscarry…so let’s say out of the 120 pregnancies about 100 women will go to term.
- If the risk of uterine rupture is only 5% then you would only see about 5 uterine ruptures.
So a doctor would have to do 300 Essure reversal surgeries to have 5 patients who had rupture of the uterus.
Our point is if you would have to do 300 Essure reversal surgeries to see 5 uterine ruptures. For a physician to start observing occurrences and differences they often have to do a lot of procedures before they can see enough bad outcomes.
If a doctor tells you their technique does not increase the risk of rupture then they:
- Have a superior surgical procedure.
- Have not done enough procedures to notice the bad results.
- Don’t keep in touch with their patients enough to know the outcomes.
If they have a superior surgical technique then they should publish their results to be reviewed by other medical professionals, and, if proven to be true, shared for the benefit of other medical professionals and other patients.
Our experience with Essure removal: 925 and counting!
Since 2009 we have performed approximately 925 surgeries to remove/reverse Essure sterilization. Although to some people this number may not seem like a lot, you should understand most Ob/Gyns have never removed Essure. Some may have done less than 10 to 20 removals to date.
When a doctor performs close to 1,000 surgeries…that gives them a lot of experience and a lot of knowledge.
C-section and Essure reversal: Death and taxes!
 You only need to do two things in life: die and pay taxes.
You only need to do two things in life: die and pay taxes.
Some people even figure out a way to not pay taxes…but we all will die. We cannot cheat death.
We tell our patients we live in a free country. You can do whatever you want as long as it does not endanger the health and wellbeing of another individual.
We recommend a c-section before going into labor…but the decision on how to deliver is between you and your doctor.
We give patients our recommendations. We provide their doctors with a copy of the Essure reversal operative note and a letter of our recommendations. We can only give you advice. We cannot live your life. Only you and your doctor can decide what is best for you.
Some doctors tell their patients they can have a vaginal birth after Essure reversal. Although this is true, it seems some of these doctors try to minimize the risk to attract more patients.
Unfortunately many reversal doctors dont have a good idea of what happens to their patients after these patients leave their office.
Most doctors try to back up their advice up with statistics from published medical studies. If there are no reliable statistics then doctors should try to publish a study documenting the answers to the important questions.
If we can’t provide reliable statistics then at least we should admit we cannot and call our recommendations ‘expert advice’.
If a doctor tells you something is safe then they should be able to quote published studies proving it or publish the results of their patient outcomes to prove that it is safe.
If a doctor’s office does not answer the phone when you call or if they don’t call you after surgery or follow up with you years after surgery or if they don’t have a way for their patients to report their pregnancies, births, or outcomes then how would anyone expect them to have reliable data on a subject of serious concern?
You only have to do two things in life: die and pay taxes. Having a c-section is not one of the required things in life!
It is possible to have a vaginal birth but…if you do…our patients and their doctor’s know the risk.
Vaginal birth after Essure reversal
We have had several patients have vaginal births after C-section. The important thing you must understand is these patients and their doctors understood the risks.
We call this giving proper informed consent…remember it is a free country and you can do what you want as long as you do not impinge upon the freedoms of another individual.
Ob/Gyn Doctor Travels to A Personal Choice For Essure reversal

No distance is too far to get the best chance of miracle! After endless research we traveled all the way from Iceland to have Dr. Monteith do my Essure reversal.
We had a fullterm, healthy baby born 10 months after reversal.
Thank you, Dr. Monteith and your amazing staff, for making the impossible possible.
Patient age: 39
Tubal ligation type: Essure
Patient hometown: Gardabaer, Iceland
The above testimonial was from an Ob/Gyn doctor who traveled to A Personal Choice for reversal of Essure sterilization. She did extensive research and thought her best chances for a successful Essure reversal was with our center.
Also we like to point out…she was an educated doctor and she knew we would provide her with the best chance for a successful Essure reversal and the best statistics on chance and risk of pregnancy after Essure reversal.
We advised her the same thing we advise all our patients: We recommended a planned c-section to minimize the risk of uterine rupture after Essure reversal.
She said she understood the risk but wanted to have a vaginal delivery. She had a safe uncomplicated vaginal delivery and both her and her baby were healthy.
Here is what you need to understand.
She was an educated Ob/Gyn doctor. She fully understood the risk and was comfortable with the risk. She also had her Ob/Gyn partner immediately next to her the entire time she was in labor and the labor and delivery suite was prepared to do an immediate C-section if required.
Most patients are not going to get the same level of one-on-one care that our Icelandic Ob/Gyn Essure reversal Doctor patient did unless they have a careful conversation with their health care team before going into labor.
Vaginal birth of twins after Essure reversal!
The following testimonial was notable because one of our Essure reversal patients had twins. She, like all of our patients, was advised to have a planned c-section.
She felt it was in her best interest to have a vaginal birth. The fact that she had twins is notable because her uterus was stretched even more with two babies compared to women who have only one baby. The fact she had twins greatly increased the stress on her uterus and the fact she did not have a uterine rupture was notable and may be reassuring to some women who have had Essure reversal.

Testimonial from patient with twins after Essure reversal.
I had my Essure removal procedure completed by Dr. Monteith in November of 2014.
I am writing to report that I got pregnant three months later and just gave birth to twin boys through an all natural vaginal birth.
I thought you’d like this information for your records, but I do wish to remain anonymous if you share it.
Wishing you the best.
Patient age: 36
Tubal ligation type: Essure sterilization
Vaginal birth of Essure reversal baby
 Here is another patient who had a vaginal birth after Essure reversal.
Here is another patient who had a vaginal birth after Essure reversal.
Dr. Monteith
I was blessed to be able to have baby Jazlyn vaginally without complications. She is truly a joy to our family.
Patient age: 27
Tubal ligation type: Essure
Patient hometown: Plainfield, Indiana
Essure reversal: Advice From Dr Monteith
As you can see from the testimonials above, you can have Essure reversal, successful pregnancy, and a vaginal birth.
It is not impossible…it is just not recommended. The video below provides more information directly from Dr. Monteith about surgery to reverse Essure.
Any surgery that makes an incision on the uterus can increase the risk of uterine rupture in a future pregnancy.
The higher the incision is made on the uterus then the higher the risk of uterine rupture. The longer you go in pregnancy, if you have multiples, or if you go into labor then that also increases the concern and risk of experiencing a uterine rupture.
Why go through so much to obtain success only to risk losing it at the very end?

