Essure Removal Surgery
Using A Uterine Tourniquet
When performing Essure removal surgery, we use a uterine tourniquet. This practice makes Essure removal surgery easier, safer, and allows us more precision during coil dissection.
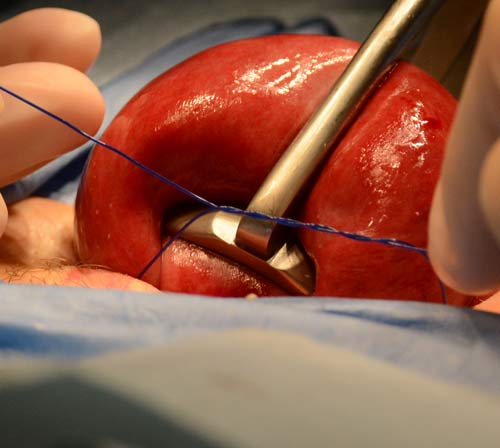
Placement of uterine tourniquet before Essure removal.
A uterine tourniquet allows better hemostasis during Essure removal surgery. Better hemostasis decreases surgeon anxiety.
Our visualization is better when hemostasis is adequate. Better visualization allows for a more precise dissection of the Essure micro-insert.
Decreased blood loss helps us keep Essure removal surgery outpatient.
In our experience, all of the above factors greatly increase our ability to remove the devices intact and with less chance of micro-insert fragmentation.
Decreasing blood loss during Essure removal surgery
We have avoided pharmaceutical attempts at hemostasis during Essure removal surgery because we feel most of these hemostatic agents don’t provide effective hemostasis and have effects upon the patient which are not conducive to early ambulation required for outpatient surgery.

Blood loss at time of peritoneal closure.
We have performed Essure removal surgery both with and without uterine tourniquets. We feel a uterine tourniquet increases the chance of intact device removal. Before placing a uterine tourniquet openings underneath each tube and in each broad ligament are created.
Initially we used a sized 14 French latex Foley catheter. We were able to put adequate tension with a low incidence of breakage when applying the Foley tourniquet. The latex material provided good compression, exhibited good knot holding characteristics, and provided adequate hemostasis during Essure removal surgery.
We then felt it was important to make our facility ‘latex free’ and we had to abandon latex catheters as uterine tourniquets. Non-latex catheters did not maintain tension during tourniquet application and hemostasis was suboptimal.
Adequate tourniquet with excellent hemostasis
We have used several different types of suture for tourniquets: chromic, non-absorbable monofilament and absorbable monofilament.
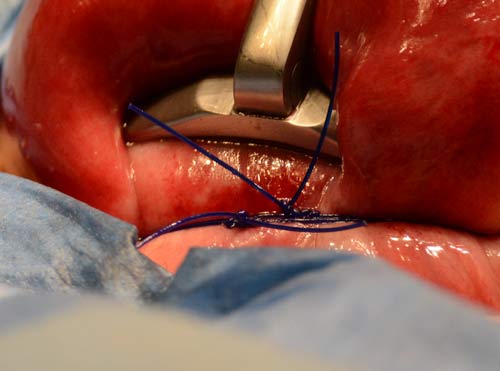
Double uterine tourniquet demonstrated.
Size 1 Chromic worked well and maintained tension during surgery; however, chromic did not exhibit a high enough tensile strength and would often break during knot tying.
Size 1 non-absorbable monofilament had a high tensile strength and could withstand tying; however, this suture was unable to maintain compression when knot tying despite using a standard surgeon’s knot and even triple throws when tying the first knot. Hemostasis was less guaranteed with non-absorbable suture.
Size 1 absorbable monofilament had great tensile strength and the suture also ‘bound more to itself’ and maintained tension during knot application. We now exclusively use 1 absorbable monofilament for uterine tourniquets during Essure removal surgery.
Essure removal surgery: Kelly forceps
It is easier to apply a uterine tourniquet with a Kelly forceps in some situations. When pelvic exposure is limited due to patient obesity or fasical scarring due to previous surgery and the uterus cannot be elevated above the rectus fascia.
The tip of the Kelly forceps allows you to apply controlled force to the tourniquet and in an adequate direction within the limited confines of the pelvis. It is advisable to wrap the suture around the tip of the Kelly forceps several times to prevent slippage. The surgeon should always provide carefully controlled force to minimize injury to the pelvic blood vessels should the tourniquet break or the Kelly forceps slip during tourniquet application.
We usually attempt to apply two tourniquets rather than one. Often the second tourniquet can provide more compression than the first tourniquet. This is readily visible when the first tourniquet becomes loose after the second tourniquet is applied.
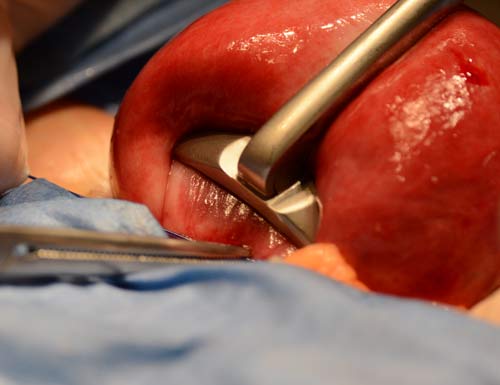
Application of Collins forceps demonstrated.
Essure removal surgery: Collin uterine forceps
A Collin uterine forceps is a valuable tool to help manipulate the uterus and provide additional compression and hemostasis. The Collin forceps should be applied first and the tourniquets second.
If applied in opposite order (uterine tourniquet and the Collin forceps) the Collin forceps will provide adequate anterior posterior compression but may decrease compression from the uterine tourniquets as uterine volume is displaced upward. Hemostasis may be less when this occurs.
Care must be taken not to entrap the ampullary segment of the fallopian tube, the ovaries, small intestines, or bladder when applying the tourniquets and the Collin forceps during the beginning of Essure removal surgery.
