







Editorial Published in The Triangle Physician April 2010
Tubal ligation is the second most frequent birth control method, chosen by more than 12 million American women. Each year 650,000 female sterilizations are performed in the US. Although tubal sterilization is considered a permanent form of contraception, many women regret their decision and would like to have their fertility restored. The most common reason for this is remarriage.
Tubal Reversal Regret
In the 1995 National Survey of Family Growth, women who reported having a tubal ligation were asked, “As things look to you now, if your tubal ligation could be reversed safely, would you want to have it reversed?” Nearly 25 percent of women with a tubal ligation expressed a desire for reversal of the operation on the part of herself, her husband or partner, or both.
In the U.S. Collaborative Review of Sterilization (CREST), women were interviewed for up to 8-14 years after the sterilization operation. At each interview, they were asked, “Do you still think tubal sterilization as a permanent method of birth control was a good choice for you?” Overall, 13% of women said they did not think that the tubal ligation was a good choice. The percentage expressing regret was 20% for women aged 30 years or younger at the time of sterilization compared with 6% for women older than 30 years at the time of tubal ligation. For women under age 25, the rate 40%. The regret rate was higher for women who were not married at the time of their tubal ligation or when tubal ligation was performed less than a year after delivery. Women who had experienced changes in marital status were 3 times more likely to seek information about tubal ligation reversal than those whose marital status had not changed.
It appears that a small percentage of women who regret having a tubal ligation and would like to have it reversed undergo tubal reversal surgery. One reason is the lack of insurance coverage for sterilization reversal. Another is that many women receive inaccurate information about tubal reversal – such as: tubal ligation cannot be reversed; the only treatment option is in vitro fertilization (IVF); or, tubal sterilization reversal is a high cost in-hospital operation.
There are no national statistics available about the number of women having tubal ligation reversals. Locally, over 8,000 tubal reversal operations have been performed at Chapel Hill Tubal Reversal Center where the procedures are performed as outpatient surgery. Analysis of the outcomes of tubal ligation reversal are made possible with a database started in 2000 at the center that now includes more than 5000 patients. It is the largest study population of this kind. Overall, 2 out of 3 women have become pregnant after their reversal procedures. Pregnancy rates vary with age and tubal ligation method. They range from 90% for women under age 30 with tubal clip procedures to 31% for those 40 and older having had tubal coagulation (tubes burned).
The success of tubal anastomosis is directly linked to surgical experience. Since the advent of Assisted Reproductive Technology, surgical training has markedly declined, and there remain few fellowship programs in the US with meaningful numbers of surgical cases. A recent study found that most of the current Reproductive Endocrinology and Infertility fellows performed less than 10 procedures and 35% of program graduates performed no surgical tubal reversals in the previous year.
The primary benefit of tubal reversal surgery is that it has a high cumulative pregnancy rate because conception is a possibility in every subsequent ovulation cycle. Tubal ligation reversal avoids the increased risk of multiple pregnancy associated with IVF (35%) and other risks of gonadotropin stimulation of the ovaries. The primary risk of tubal reversal is the long term risk of ectopic pregnancy (10-15%).
Although tubal sterilization is meant to be permanent, the reality is that it can be reversed through cost-effective outpatient surgery.
Tubotubal Anastomosis
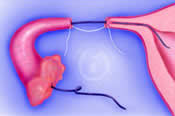 After opening the blocked ends of the remaining tubal segments, a narrow flexible stent is gently threaded through their inner cavities or lumens into the uterine cavity. This ensures that the fallopian tube is open from the uterine cavity to its fimbrial end. The newly created tubal openings are then drawn next to each other by placing a retention suture in the connective tissue that lies beneath the fallopian tubes. The retention suture avoids the likelihood of the tubal segments subsequently pulling apart.
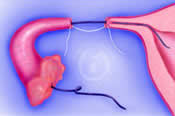
After opening the blocked ends of the remaining tubal segments, a narrow flexible stent is gently threaded through their inner cavities or lumens into the uterine cavity. This ensures that the fallopian tube is open from the uterine cavity to its fimbrial end. The newly created tubal openings are then drawn next to each other by placing a retention suture in the connective tissue that lies beneath the fallopian tubes. The retention suture avoids the likelihood of the tubal segments subsequently pulling apart.
 Microsurgical sutures are used to precisely align the muscularis and serosa while avoiding the mucosa of the fallopian tube. The tubal stent is then gently withdrawn from the fimbrial end of the tube.
Microsurgical sutures are used to precisely align the muscularis and serosa while avoiding the mucosa of the fallopian tube. The tubal stent is then gently withdrawn from the fimbrial end of the tube.
Dr. Berger is a reproductive surgeon and Medical Director of Chapel Hill Tubal Reversal Center, Chapel Hill, North Carolina.
References
1. Surgical Sterilization in the United States: Prevalence and Characteristics, 1965–95. Vital and Health statistics Series 23 No. 20, National Center for health statistics.
2. Hillis SD, Marchbanks PA, Tylor LR et al. Poststerilization Regret: Findings From the United States Collaborative Review of Sterilization. Obstet Gynec 1999 93(6): 889-95.
3. Armstrong A, Neithardt AB, Alvero R et al. The role of fallopian tube anastomosis in training fellows: a survey of current reproductive endocrinology fellows and practitioners. Fertil Steril. 2004 82(2):495-7.
