Minimally Invasive No Scalpel Vasectomy Reversal
A Step-By-Step Guide
The most recent advance in vasectomy reversal is minimally invasive No scalpel vasectomy reversal using techniques learned from No scalpel vasectomy.
Traditional vasectomy reversal involves creating a 2 to 4 inch incision in the scrotum with a scalpel: either a single incision is created in the center or two incisions are created, one on each side of the scrotum.
Minimally invasive No scalpel vasectomy reversal involves creating a single scrotal opening with an instrument specially designed to make a small opening with less skin trauma.
No Scalpel Reversal Opening

No scalpel dissector being used to create a single opening in the center of the scrotum by using a spreading motion
Minimally invasive No scalpel vasectomy reversal surgery does not require a scalpel. Instead a No scalpel dissector is used to make a single opening in the center of the scrotum using a spreading motion. Skin is very elastic and responds favorably to spreading.
A spreading dissection often results in less tissue trauma, less bleeding, and results in a smaller opening than does a dissection performed with a scalpel. A minimally invasive vasectomy reversal incision is often so small sutures are not required to close the incision.
1 to 2 cm Incision Is More Than Adequate
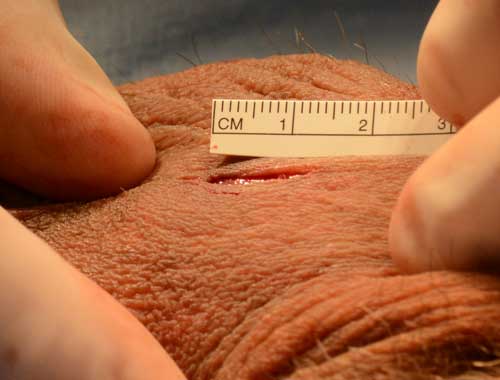
The single no scalpel opening is in the midline of the scrotum and is typically 1 to 2 cm in length.
The No scalpel dissector can be used to create an opening up to 2cm in length for reversing vasectomy. Both vasectomy sites can usually be reversed through this single opening and this amount of exposure is more than adequate to access each vas deferens and perform microsurgical vasectomy reversal.
Note the absence of blood on the surgical field.
No additional surgical steps were required to stop bleeding and no vasoconstrictive medications (medicines that decrease bleeding) were used in the skin. This provides visual evidence as to the minimally traumatic nature of this reversal procedure.
Microsurgical Vasectomy Reversal Through A Small Opening

No scalpel ring forceps securely hold the ends of the vas deferens in place during the reversal procedure.
The upper and lower divided ends of the vas deferens can be retrieved through the single center opening using no scalpel vasectomy techniques applied to vasectomy reversal.
A No scalpel rings forceps is used to locate the previous vasectomy site and to elevate the site through the scrotal incision.
The No scalpel ring forceps can then be used to secure the upper and lower ends of the vas deferens at the level of the scrotal skin for microsurgical vasovasostomy.
Microsurgical repair using Microsurgical Sutures
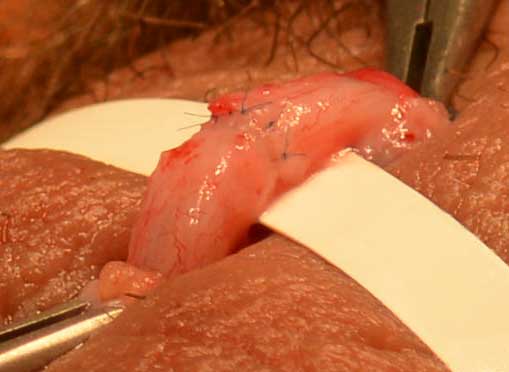
A close up view of the site of anastomosis with a ruler underneath the repair site to provide a visual backdrop.
The ends of each vas deferens can be rejoined using either 8-0 or 9-0 miscrosurgical sutures. The amount of surgical exposure provided by a minimally invasive technique is more than adequate to allow for miscrosurgical anastomosis.
The smaller scrotal skin opening also provides compression of the blood vessels during the repair and this contributes further to the minimal amount of bleeding observed during a no scalpel vasectomy reversal.
Completion of vasectomy reversal

The single No scalpel opening shown with tension placed on scrotal skin. Note the size of the opening has increased slightly as a result of obtaining access to the second repair site
These last two photos show a single no scalpel vasectomy reversal opening after the successful completion of the reversal of both vasectomy sites.
The top photo shows the opening when tension is applied on the scrotal skin.
The bottom photo shows the opening when the scrotal skin is allowed to resume its normal contractile state.
The small nature of the opening combined with the natural tendency for the scrotal skin to tighten is why this incision does not require sutures to close.

The no scalpel opening is difficult to see when scrotal skin tension is released and the scrotal skin regains its normal state. The skin opening is ‘self closing’ and will heal without the need for skin sutures.
Sutures either have to be removed by a health care provider or, if absorbable sutures are used, will require 10 to 21 days to be fully absorbed.
A no scalpel opening will typically be fully closed within 2 to 5 days without requiring any special treatment. Not requiring sutures to close the incision is a huge benefit because sutures cause more discomfort until they have either been removed or have dissolved.
Minimally invasive No scalpel vasectomy reversal offers a substantial improvement in when compared to traditional vasectomy reversal.
Minimally Invasive No Scalpel Vasectomy Reversal
Critics of minimally invasive No scalpel vasectomy reversal often argue the incision is too small to perform an adequate vasectomy reversal and the smaller incision does not allow surgeons to perform a vasoepididymostomy (bypass) procedure.
Too small of an incision. When No scalpel vasectomy was first introduced in the United States in the 1980’s many critics made the same argument about this newer vasectomy procedure. Even now many surgeons will not perform no scalpel vasectomy even though it has a much lower complication rate. Many of these same physicians also perform vasectomy reversal and continue to perform the much larger scrotal incisions they were initially trained to perform. Many of these surgeons are reluctant to step out of their comfort zone.
Too small of an incision to perform vasoepididymostomy. This is a valid criticism of minimally invasive vasectomy reversal. To adequately perform a vasoepididymostomy the scrotal incision has to be large enough to allow removal of the entire testicle so the surgeon can have access to the epididymis.
A complicated bypass procedure is only required in 4% of vasectomy reversal patients. If this is required a smaller minimally invasive incision can be enlarged during the procedure with a scalpel during the reversal to allow the surgeon enough exposure to perform vasoepididymostomy.
Most men can have their vasectomy reversed with a no scalpel mini-incision reversal technique. Why expose 96% of men to larger incisions requiring sutures when only 4% of men will require a larger incision for a more complicated by-pass procedure?
