Essure Removal
Avoid Excessive traction
 When we first began performing Essure removal, we would remove the devices using manual traction.
When we first began performing Essure removal, we would remove the devices using manual traction.
As we gained more experience, we realized the best way to reduce the risk of breaking the Essure devices was to minimize excessive traction and avoid electrodissection.
We now perform en bloc resection of Essure micro-inserts during our Essure removal procedures and this minimizes the chance of fracturing the devices and the risk of leaving Essure fragments during removal.
 Essure removal: Mini-laparotomy is our preference
Essure removal: Mini-laparotomy is our preference
We perform our Essure removal procedures under general anesthesia, as outpatient procedures, and through a mini-laparotomy abdominal incision. We feel this approach allows us better surgical control.
Although a minimally invasive laparoscopic or robotic approach is possible, we feel operating through a mini-laparotomy incision allows a more precise dissection of the Essure devices, allows us to avoid the use of excessive coagulation because we can maintain better hemostasis, and increases our tactile perception when palpating for the distal most tip of the inner coil.

Skin incision in a thin patient used to remove Essure devices using the traction method. Skin incisions for en bloc coil dissection are slightly larger to allow better exposure and uterine tourniquet placement.
Moreover our approach allows us to operate quickly and efficiently without adding increased cost because of increased operating room time and increased equipment cost when using a robotic or laparoscopic approach.
Our patients are often covering most of the cost of Essure removal and we must be more mindful of the cost of Essure removal in our practice.
Although we do perform laparotomy, all of our surgical procedures are ambulatory. We keep our incisions as small as is safely prudent and in most cases the total length of our incision is similar, or slightly longer, to the total length of the three (3) to four (4) incisions made during minimally invasive surgery.
 Essure removal: Minimizing traction
Essure removal: Minimizing traction

Initially we would remove Essure coils with direct traction. To accomplish this we would locate the distal most portion of the Essure device with digital palpation.
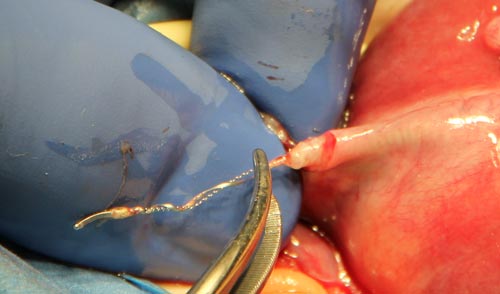
Using sharp dissection with a scalpel, we would make an incision into the isthmic section of the fallopian tube and locate the lateral end of the Essure micro-insert.
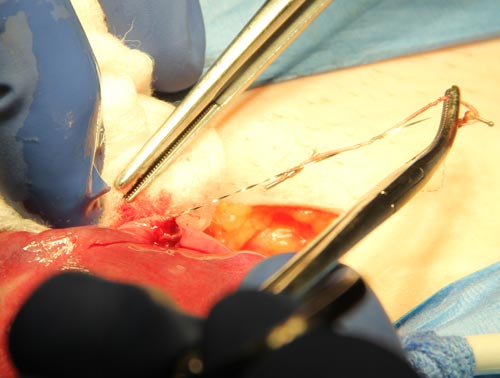
Once the lateral end of the micro-insert was identified we would apply manual traction with a hemostat. Once the device would elongate, we would apply a second hemostat and using a ‘hand-over-hand’ technique we would gradually remove the Essure device using steady traction.
 We found larger forceps (i.e. Kelly forceps) to be more damaging to the micro-inserts and smaller forceps (i.e. Debakey) did not provide enough gripping strength.
We found larger forceps (i.e. Kelly forceps) to be more damaging to the micro-inserts and smaller forceps (i.e. Debakey) did not provide enough gripping strength.
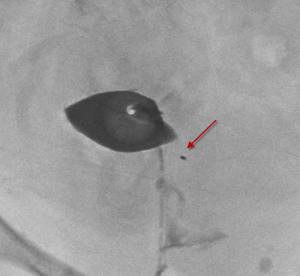
This method worked well but we soon realized approximately 1 out of 10 patients would have a fracture of the outer coil at the proximal most portion during removal.
These patients would often be left with a small fragment of the proximal most rectangular radiographic marker. This platinum band is welded to the outer nitinol coil and seems to be a source of weakness in the outer coil.
Removing Essure: Reducing the risk of coil fracture
We feel manual extraction of the micro-insert device increases the risk of outer coil fracture. Manual extraction may be more appropriate for micro-inserts that do not have significant amounts of fibroelastic tissue in-growth.
En bloc surgical dissection allows for more intact coil removal along with surrounding fibroelastic tissue.
